Reference Architecture
0.1.0 - release
![]()
Reference Architecture
0.1.0 - release
![]()
This page is part of the Reference Architecture (v0.1.0: Releases Draft) based on FHIR (HL7® FHIR® Standard) R4. This is the current published version. For a full list of available versions, see the Directory of published versions
In the development of Reference Architecture, the following areas are to be considered:
Architectural documentation shall follow the WHO SMART Guideline methodology which structures digital health documentation into the following components:
The primary focus will be creating the L3 artifacts necessary for the realizing of prioritized digital health workflows and a set of tests that can be utilized by digital health vendors to determine the adherence of their products to that infrastructure. In some cases, the L2 artifacts may not be fully developed and the architects will contribute to the development of these artifacts in coordination with appropriate subject matter experts.
For the production of content, we utilize the HL7 FHIR IG Publisher as the main publication tool for the development of architectural content. In particular, the Authoring L3 Content.
The Digital Adaptation Kits (DAKs) provide a structured set of business requirements for digital health applications. While some of these artifacts will be or are already being developed using standards for business requirements (e.g. BPMN, DMN tables) this artifacts are primarily designed for accurate representation of business needs from subject matter experts by business analysts. We are developing tooling to automate or ease the development of corresponding L3 artifacts in terms of HL7 FHIR Resources.
One essential component of this is the definition and representation of the appropriate requirements (as FHIR Requirements resources) and system or human actors (as FHIR ActorDefinition resources). (Draft) examples include:
Another essential component are the generic business processes and workflows (which we are standardizing to BPMN diagrams for computability). These workflows outline the main functionality needed for the actors/generic personas. The Reference Architecture shall define the digital health infrastructural components and necessary transactions (e.g. messages sent via APIs) to realize these workflows.
THe reference architecture adopts the normative words defined in IETF Best Current Practice 14: Key words for use in RFCs to Indicate Requirement Levels (BCP-14) (currently RFC 2119 and RFC 8174, certain words indicate whether a specific content of the Technical Framework is normative. The key words "MUST", "MUST NOT", "REQUIRED", "SHALL", "SHALL NOT", "SHOULD", "SHOULD NOT", "RECOMMENDED", "MAY", and "OPTIONAL" in this document are to be interpreted as described in RFC 2119. Informative content does not contain these key words.
The Reference Architecture SHALL make us of open standards which are maintained by a Standards Development Organization (SDO) with an open partiicipation policy and whhich are unencumbered by license restrictions that would limit the implementation. This use of standards SHALL apply to:
The Reference Atchitecture will make use of global best practices and open standards where available. If not available we will:
When describing the data needs for a use case or transaction, the use of Logical Models is highly encouraged. These can then be mapped to relevant data models (e.g. HL7 FHIR R4).
In consideration of the:
the identification of relevant of HL7® FHIR® syntactic standards for the representation and exchange of health information will be prioritized.
In the case that there are alternative open standards to meet sub-domain specific business requirements (e.g. DICOM, OMOP), such standards will be considered with a reflection on:
The use of fully open, normative terminolgies SHALL be utilized where avaiable and relevant to the use case. The termonolgies, in order of priority, include:
The utilization of terminologies for specific health content areas (e.g. HIV, Immunizations) is subject to the general SMART Guidelines' Standard Operating Procedures for the development of https://smart.who.int/ig-starter-kit/l2_dak_authoring.html.
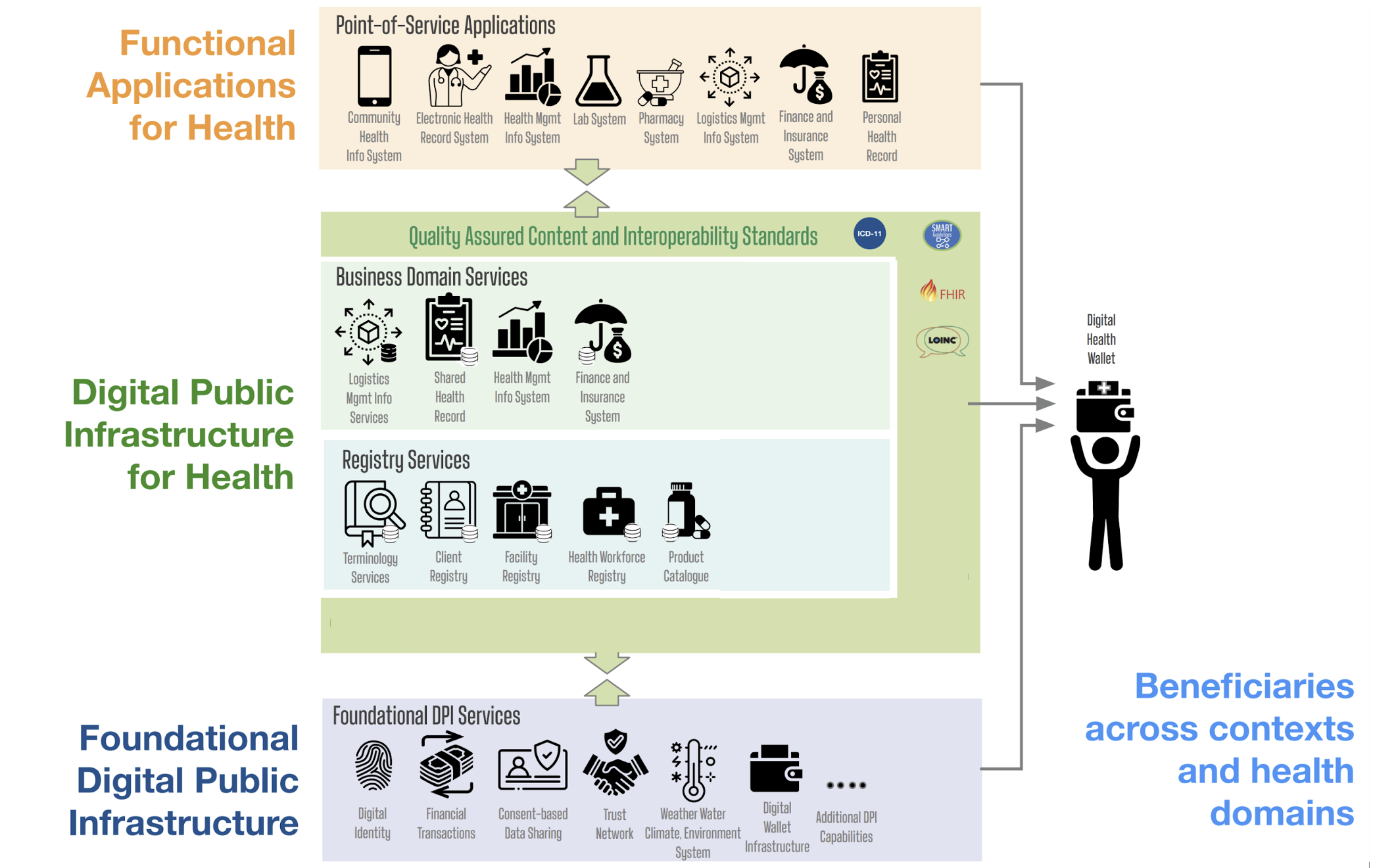
The Reference Architecture draws from the OpenHIE architectural components, in particular the Business Domain Services & Registry Services.
==To Do:== review OpenHIE components and include them, refining as necessary, into the Reference Architecture.
These components should be brought into the architecture by identifying a specific requirement or workflow coming from a DAK.
https://docs.github.com/github/writing-on-github/getting-started-with-writing-and-formatting-on-github/basic-writing-and-formatting-syntax ==To Do:== add your name The following people are contributing to the core architecture